Article Text

Abstract
Background: Exposure to cleaning products has frequently been reported as a symptom trigger by workers with work-related asthma diagnosed in workers’ health clinics in the city of São Paulo, Brazil.
Objectives: To estimate rhinitis and asthma symptoms prevalence and to analyse associated risk factors.
Method: A respiratory symptoms questionnaire (Medical Research Council 1976) and the International Study of Asthma and Allergies in Childhood questionnaire were applied to 341 cleaners working in the city of São Paulo, along with obtaining full occupational histories, skin prick tests and spirometry. Timing their symptoms onset in relation to occupational history allowed estimation of work-related asthma and/or rhinitis. Risk factors related to selected outcomes were analysed by logistic regression.
Results: 11% and 35% of the cleaners had asthma and rhinitis, respectively. The risk of work-related asthma/rhinitis increased with years of employment in non-domestic cleaning (OR 1.09, 95% CI 1.00 to 1.18, >0.92–3 years; OR 1.28, 95% CI 1.01 to 1.63, >3–6.5 years; OR 1.71, 95% CI 1.02 to 2.89, >6.5 years). Atopy was associated with asthma and rhinitis (OR 2.91, 95% CI 1.36 to 6.71; OR 2.06, 95% CI 1.28 to 3.35, respectively). There was a higher risk of rhinitis in women (OR 2.07, 95% CI 1.20 to 3.70).
Conclusions: Cleaning workers are at risk of contracting work-related asthma and/or rhinitis, and the risk increases with years of employment in non-domestic cleaning. Women present higher risk of rhinitis than men.
- ECRHS, European Community Respiratory Health Survey
- FVC, forced vital capacity
- FEV1, forced expiratory volume in one second. ISAAC, International Study of Asthma and Allergies in Childhood
Statistics from Altmetric.com
- ECRHS, European Community Respiratory Health Survey
- FVC, forced vital capacity
- FEV1, forced expiratory volume in one second. ISAAC, International Study of Asthma and Allergies in Childhood
According to the World Health Organization, the prevalence of asthma has been increasing over recent decades. It is reaching epidemic levels and affecting young populations, with a serious economic and social impact.1
Multicentre studies have shown that the prevalence of current asthma among adolescents (13–14 years old) ranges from 2% to 37% worldwide.2 In Brazil, the prevalence has been estimated to be 9% to 27% in seven urban centres3 and 21% in São Paulo.3 The natural history of asthma suggests lower prevalence among adults. In a predominantly Western Europe large multicentre study on young adults, the prevalence of asthma was estimated to be 4% to 32%.4 A population-based study on young adults (aged 23–25 years) in the State of São Paulo found an asthma prevalence of 11.8%.5
Occupation can be a risk factor for asthma in adults, either by aggravating previous asthma (work-aggravated asthma) or by causing new-onset asthma (work-related or occupational asthma). Cleaning activities seem to represent an important risk.6,7 In Finland, the mean annual incidence rate of occupational asthma in cleaners was found to be 32/100 000, compared with 17.4/100 000 for workers in general.8 The work-related attributable fraction of asthma in cleaners was 33%, with an excess risk of 50%, in comparison with workers in administrative activities.9 A case-control study showed that female cleaners had a risk of asthma 42% higher than controls.10 In the city of São Paulo, cleaning was the main occupation in terms of the number of cases of occupational asthma among women, and cleaning products were the most frequently reported agent, between 1995 and 2000.11 In a surveillance programme in the US, cleaning products were also associated with numerous cases of work-related asthma, especially among cleaners.12
Studies have shown that asthma and rhinitis often coexist, and that allergic rhinitis usually precedes the onset of asthma. As with asthma, the prevalence of rhinitis seems to be increasing. The range of reported allergic rhinitis is 2–21%13 and, while the exact prevalence of non-allergic rhinitis is not known, estimates have indicated that the rhinitis in 20–50% of such patients actually has non-allergic causes.14–16 Many types of occupational exposure are associated with rhinitis, because it shares the same aetiological agents with asthma.17 Both non-allergic and mixed rhinitis (combination of non-allergic and allergic rhinitis) occur more frequently in adults than in children, and are more common in women.18
The objectives of the present study were to measure rhinitis and asthma symptom prevalence in cleaners and to analyse associated risk factors.
METHOD
Study design
This was a cross-sectional study on the prevalence of airway symptoms with an internal comparison of work-related asthma/rhinitis prevalence according to years of employment in non-domestic cleaning.
Study population
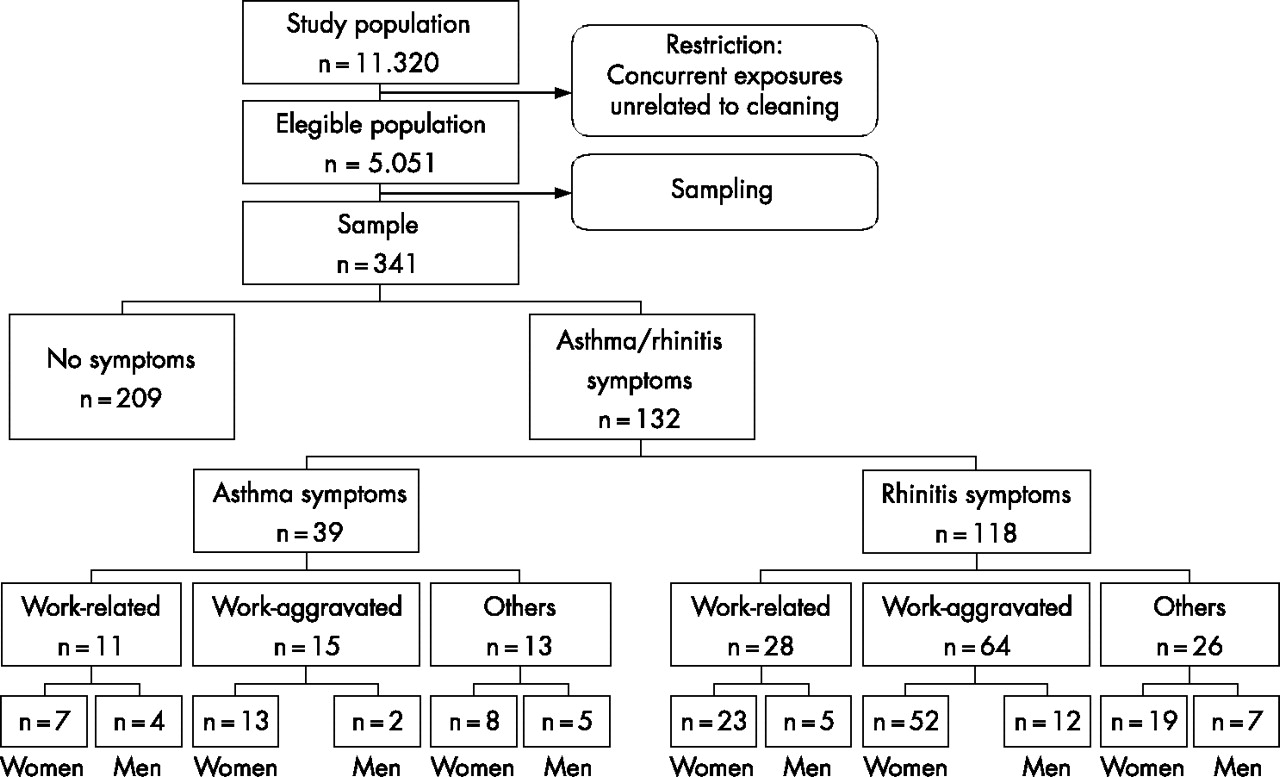
The Cleaning Service Company Workers’ Union of the southern zone of São Paulo supplied a list of workplace addresses, with the names of the cleaning companies and the respective size of the cleaning team in each location, giving a total of 11 320 workers. All locations with possible airborne dust, fumes or gases unrelated to cleaning activities, such as transportation, industrial plants, hospitals and healthcare establishments, parks, clubs, stadiums, bars and nightclubs were excluded, leaving 5051 workers available for sampling. The suitable sample size was calculated in accordance with a conservative method (p = 0.50; 95% confidence level, 0.05 error sampling). Based on the location and total number of cleaners at each place, a proportional sample was selected by systematic sampling. Distribution by economic activity was respected. Taking into account the information on employers, all the cleaners from the selected locations were assessed. Five pregnant women were excluded from the sample, as this condition is associated with changes in pulmonary function. Thus, the study population comprised 341 subcontracted cleaners employed by 32 cleaning service companies, working in 36 locations (fig 1). The ethics committee of the School of Public Health of the University of São Paulo granted approval for the study, and data were collected from December 2002 to May 2003.

Flow chart for selecting the population for a cross-sectional study among workers employed in non-domestic cleaning.
Questionnaires
Symptoms
Information on respiratory symptoms was collected using a translation of the Medical Research Council (MRC)19 questionnaire and International Study of Asthma and Allergies in Childhood (ISAAC) asthma and rhinitis modules. The asthma module had previously been validated in Portuguese.20 Additionally, information about symptoms onset and cleaning-related airway symptoms were obtained.
Exposure assessment
Information on the workers’ employment histories and the characteristics of their current non-domestic cleaning work was obtained by means of a modified job-specific questionnaire that had been used within the European Community Respiratory Health Survey (ECRHS). The length of employment in non-domestic cleaning was obtained from these full occupational histories. The frequencies of performing six different cleaning tasks and using 19 different cleaning products at the time of the interview were recorded as times per week, times per month, or times per year. A question about inhalation accidents involving vapours, gases or fumes was included.
Skin prick tests
Skin prick tests were performed using a panel of nine allergens: Dermatophagoides farinae (100 BU/ml), Dermatophagoides pteronyssinus (100 BU/ml), Blomia tropicalis (not standardised), Periplaneta americana (1%), Blatella germanica (1%), cat epithelium (100 BU/ml), dog epithelium (100 BU/ml), pollen (100 BU/ml) and Aspergillus fumigatus (5%) (Prickit - FDA Allergenic/Alk Abelló). A positive response was defined as a mean wheal diameter 3 mm larger than negative control, read after 20 min.21
Pulmonary function
Spirometry was performed using an electronic pneumotachograph (Koko pneumotach spirometer, PDS Medical Instruments, Louisville, USA), in accordance with the American Thoracic Society recommendations.22 Analyses were performed on the largest forced vital capacity (FVC) and forced expiratory volume in one second (FEV1) curve, and expressed as percentages of the predicted values for the reference Brazilian population.23
Definitions
Asthma: a score of five or more points, as defined in a previous validation study using the ISAAC asthma symptoms questionnaire among adults.20
Rhinitis: self-reported sneezing or runny or blocked nose, without cold or flu over the past 12 months.
Chronic bronchitis: morning productive cough for at least three months a year, for two consecutive years.
Atopy: positive skin prick test for at least one of nine common allergens.
Cleaning-related airway symptoms: if something at work caused at least one of the following symptoms: dry cough, productive cough, wheeze, chest tightness, or shortness of breath (cleaning-related lower airway symptoms); sneezing, runny nose, blocked nose, or nasal burning (cleaning-related upper airway symptoms).
Work-aggravated asthma: asthma with wheezing starting before working in non-domestic cleaning, and with cleaning-related lower airway symptoms.
Work-aggravated rhinitis: rhinitis with nasal symptoms starting before working in non-domestic cleaning, and with cleaning-related upper airway symptoms.
Work-related asthma: asthmatics with new-onset wheezing after starting working as non-domestic cleaning workers, and with cleaning-related lower airway symptoms.
Work-related rhinitis: rhinitics with new-onset nasal symptoms after starting working as non-domestic cleaning workers, and with cleaning-related upper airway symptoms.
Inhalation accidents: occurrence at any time in the past of inhalation of significant quantities of vapours, gases, fumes or dust that led to immediate respiratory symptoms (within 24 h).
Statistical analyses
Due to the small sample size, we grouped the cases of asthma with rhinitis for some of the analyses, thus classifying three groups according to different health outcomes: no symptoms (reference), asthma/rhinitis symptoms and, from the latter, a subgroup with work-related asthma/rhinitis. Demographic, respiratory health and occupational characteristics of the participants, divided by sex, were tested using the χ2 or Student’s t test to identify different profiles between health outcome groups. The Cochran–Armitage test for trend was applied to examine the effect of length of employment in non-domestic cleaning for health outcomes. The number of years of employment in non-domestic cleaning was divided into quartiles: first quartile: up to 0.92 years; second quartile: more than 0.92 and up to three years; third quartile: more than three and up to 6.5 years; and fourth quartile: more than 6.5 years. Unadjusted odds ratios (ORs) and 95% confidence intervals (95% CIs) were calculated, by sex, for work-related asthma/rhinitis according to daily current use of cleaning products or performing of cleaning tasks, using two categories of exposure levels (fixed cut-off of three times/week), with the low exposure level as reference. Unconditional logistic regression models24 were run to evaluate ORs and 95% CIs for asthma/rhinitis, adjusted for the following variables: age, gender (male as sex reference group), atopy, smoking, number of years of employment in non-domestic cleaning (first quartile as low exposure reference group) and inhalation accidents. For all tests, p⩽0.05 was considered significant. Data analyses were performed through the use of SAS software.25
RESULTS
Seventy per cent of the study participants were women. Compared to men, women were older (36.3 (9.1) vs 32.4 (10.4); p = 0.0007), had worked in non-domestic cleaning for longer time (5.6 (5.5) years vs 2.9 (3.8) years; p<0.0001) and had had more inhalation accidents (13.1% (n = 32) vs 4.2% (n = 4); p = 0.016). The means of the expected values for FVC% and FEV1% were 82.6% and 84.2%, respectively, among women; and 94.2% and 93.9%, respectively, among men.
Table 1 presents the demographic, clinical and occupational characteristics of the study population for the women and men separately, according to the presence of rhinitis and/or asthma symptoms. In relation to the women without symptoms, the women with asthma/rhinitis presented with a greater proportion of current smoking and atopy and lower FEV1/FVC%, and more cleaning-related airway symptoms. Furthermore, they had greater prevalence of chronic bronchitis and inhalation accidents, but neither of these was statistically significant. Among the women with work-related asthma/rhinitis, the prevalence of atopy was significantly greater and, even though fewer of these women had previously worked in domestic cleaning, they had remained in the cleaning profession (both domestic and non-domestic) for a longer time and had had more inhalation accidents than the women without respiratory symptoms. The women with work-related asthma/rhinitis also presented a higher proportion of current smoking and lower FEV1/FVC%, but without reaching significance.
Demographic, respiratory health, and occupational characteristics of the study population, São Paulo Metropolitan Area, 2003
The men with asthma/rhinitis symptoms had significantly more cleaning-related airway symptoms than did the reference group. Among these men with asthma/rhinitis symptoms, there was a greater prevalence of atopy, lower FEV1/FVC%, more former domestic cleaning workers (as housekeepers, for example), and more inhalation accidents (without significance). More men with work-related asthma/rhinitis had worked in professional domestic cleaning. This group presented lower FEV1/FVC% and more atopy, although without statistical significance.
Approximately 56% (n = 192) of the workers reported cleaning-related airway symptoms (positive response to the question: “Has something at work caused at least one of the following symptoms: dry cough, productive cough, wheeze, chest tightness, shortness of breath, sneezing, runny nose, blocked nose or nasal burning?”). The symptoms could be related to more than one agent, and each agent could be related to more than one symptom, thus resulting in 625 citations. The symptoms most frequently cited were: sneezing (30%), nasal burning (16%) and dry cough (15%). A majority of the citations (63%) referred to upper airway symptoms (tables 2 and 3). The agents most frequently mentioned were chlorine/bleach (25%) and dust (20%).
Cleaning agents related to upper airway symptoms, São Paulo Metropolitan Area, 2003
Cleaning agents related to lower airway symptoms, São Paulo Metropolitan Area, 2003
The general prevalence of asthma was 11% (fig 1), without any difference between the men and women. Twenty five per cent (7/28) of the asthma cases among women and 36% (4/11) among men were work-related asthma. The proportion of asthma aggravated by the work was 46% (13/28) for the women and 18% (2/11) for the men.
There was a significant difference in the prevalence of rhinitis between the women (38%) and the men (25%), p = 0.009. Twenty five per cent (23/94) of the cases of women with rhinitis were work-related. The proportion of work-related rhinitis among the men was 20% (5/24). Among the women with rhinitis, the prevalence of rhinitis aggravated by the work was 55% (52/4), while among the men it was 50% (12/24).
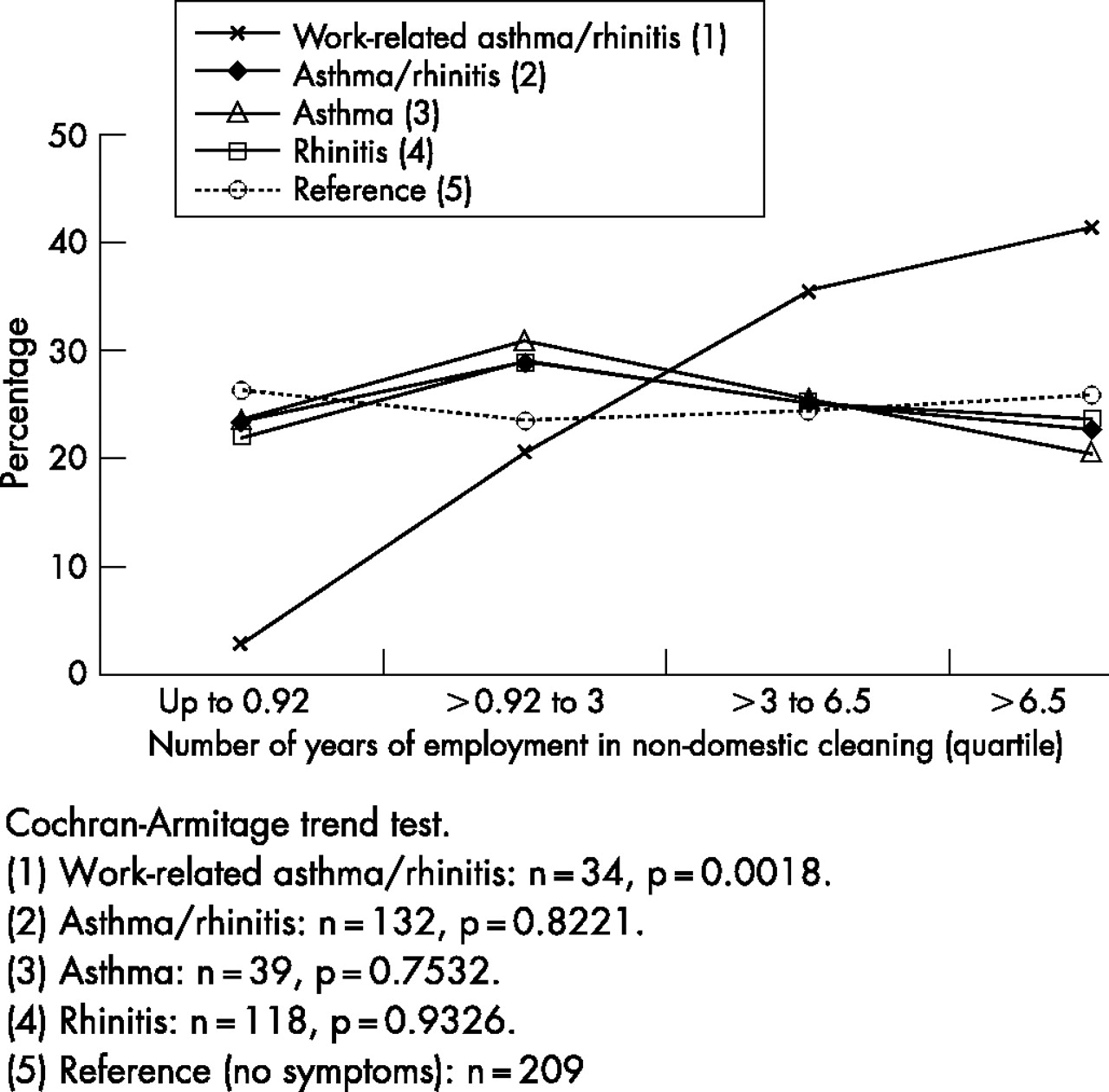
A significant linear trend of increasing prevalence of work-related asthma/rhinitis with increasing number of years of working in non-domestic cleaning was observed (p = 0.0018) (fig 2). Separately, this trend was seen for work-related rhinitis and for work-related asthma, although the latter was not significant (data not shown). Thus, the prevalence of work-related asthma/rhinitis ranged from 3% among the workers with less than one year in non-domestic cleaning to 41% for those with 6.5 years or more.
{kind=link}
{kind=link}
Trend test for prevalences of general and work-related asthma and rhinitis, according to the quartile of number of years of employment in non-domestic cleaning, São Paulo Metropolitan Area, 2003.
Using the group that performed tasks or used products less than three times a week as the exposure reference and the group without asthma or rhinitis symptoms as the symptoms reference, most of the tasks performed and products used presented similar frequencies for the workers with work-related asthma/rhinitis and those without symptoms (table 4). The commonest tasks were those involving washing floors, removing dust and using chlorine/bleach, disinfectant, detergent/liquid soap and multiuse products. Among the men, a significant association between the use of ammonia and work-related asthma/rhinitis was identified.
Unadjusted odds ratios and 95% confidence intervals for work-related airway symptoms and current daily tasks performed and use of cleaning products, São Paulo Metropolitan Area, 2003
Finally, in the unconditional logistic regression model, the main individual exposure factors have been included to show their influence on the occurrence of the respiratory effect (table 5). The female gender showed a strong association with rhinitis. Atopy was also associated with asthma and rhinitis. Smoking was consistently associated with asthma symptoms. The risk of work-related asthma/rhinitis was 71% higher for those with more than 6.5 years in the activity.
Multivariate associations (adjusted odds ratios and 95% confidence intervals) for general and work-related asthma/rhinitis, and risk factors, São Paulo Metropolitan Area, 2003
DISCUSSION
This cross-sectional study of a cleaning workforce was designed to measure rhinitis and asthma symptom prevalence, and to analyse associated risk factors. The lack of a reference population and the study design do not allow us to state whether there is an excess of airway symptoms in this population. However, the risk of work-related asthma/rhinitis symptoms increased with the length of employment in non-domestic cleaning. The small number of cases prevented us from assessing odds ratios for work-related asthma and work-related rhinitis separately. Our results reinforce previous studies in which cleaning activities were associated with work-related asthma,7 and studies that found an excess risk of asthma among cleaners.6,9,10
The asthma prevalence found in this study (11%) was slightly lower than what was found among cleaning workers from 14 countries (14%).26 The proportion of possible work-related asthma cases found in our study (25% for women) is consistent with a previous population-based study that showed that around 30% of the asthma cases among cleaning women may be a reflection of occupation-derived asthma.9 Although no difference in asthma prevalence was identified between men and women, the expected FEV1% and FVC% values for the women were close to the lower limit, and lower than the corresponding values for the men, despite being within the range of normal values. Considering the relation that was found between length of time working in non-domestic cleaning and the risk of work-related asthma/rhinitis, one possible explanation for these lower values found could be the greater length of exposure among the women (5.6 (5.5) vs 2.9 (3.8) years, p<0.0001). It must also be remembered that domestic cleaning in these workers’ own homes, which is generally attributed to the women, may be another source of exposure. The hypothesis of a dose-response relation between cleaning activities and respiratory symptoms that is suggested by this reasoning is consistent with the findings from a cross-sectional study among domestic employees in Spain, in which despite the lack of an association between exclusively non-domestic cleaning and respiratory symptoms, the subjects who reported simultaneous employment in domestic and non-domestic cleaning were at increased risk.27 Similar findings were also shown in a subsequent case-control study, in which current or former employment in non-domestic cleaning was strongly and independently associated with symptoms of asthma and chronic bronchitis.28 It was not possible for us to assess the risk of simultaneous employment in domestic and non-domestic cleaning, because less than 5% of our subjects declared having a second cleaning job. This is explained by the fact that in Brazil, non-domestic cleaners have a working week of 44 h, which is different from the situation in the Spanish population, in which 80% of the female non-domestic cleaners work part-time, for an average of 20 h/week.29 Therefore, independent of any differences relating to how the domestic and non-domestic work is organised, or to qualitative and quantitative differences in cleaning products and procedures from one country to another, the role of elements present in cleaning activities that induce or aggravate airway symptoms is evident.
The published literature confirms that both the allergic and non-allergic categories of rhinitis may precede the onset of asthma.30,31 Therefore, identifying the rhinitis symptoms may be an important measure for preventing asthma. Considering non-atopic rhinitis to be the presence of rhinitis symptoms in the absence of allergy identifiable by the skin prick test, the proportion of non-atopic rhinitis among the rhinitic population was 34% among the women and 30% among the men. The exact prevalence of non-allergic rhinitis is not known, but estimates indicate that the rhinitis of 20–50% of such patients has non-allergic causes.14–16 On the other hand, the prevalence of allergic rhinitis among cleaning workers (23%) is slightly above the upper limit of the expected range for the general population, which is 2–21%.13 We found significantly greater overall prevalence of rhinitis among cleaning women, and also an association between rhinitis and female gender. By investigating risk factors for the association between many types of occupational exposure and non-infectious rhinitis, Hellgren et al32 found that the increased risk was mainly among male cleaners. There is controversy in the findings relating to the behaviour of the airways in men and women, considering that, according to some authors,18 but not others,33 both types of rhinitis (mixed and non-allergic) occur more frequently among women. Despite this, it is worth remembering that most cleaning products are soluble in water and consequently have the capacity to irritate the upper parts of the airways. Thus, our study adds to the little previous knowledge of rhinitis prevalence rates among adults, but there remains the challenge of evaluating how much of the rhinitis among cleaning workers is non-allergic rhinitis and what role the exposure to irritants has within this context.
High atopy prevalence was found, showing a significant association with asthma/rhinitis ever. This disagrees with a previous study of asthma characteristics among European cleaning workers, in which there was lower atopy prevalence (27%) and it was suggested that it was unlikely that IgE-dependent mechanisms had a predominant role in cleaning-related asthma.26 One of the most common tasks among Brazilian cleaners was dusting/sweeping, and 18% of them reported dust-related sneezing. In this setting, they may have been exposed to high levels of house dust mite. According to an experimental study on the adjuvant effect of surfactants (detergent/soap) on the production of specific IgE antibodies, using a mouse model, dust exposure added to frequent use of surfactants could facilitate sensitisation.34 Our finding of high atopy prevalence was also higher than in the ECRHS population study,32 and this may be explained by the greater number of allergens used in this present study (9 vs 4 allergens, respectively), and the measurement methods (skin prick test vs specific serum IgE, respectively). Comparing the data on D pteronyssinus alone, there was also a higher prevalence of sensitisation among the Brazilian cleaners (28%) than among the young adults in the ECRHS (19%).35 Moreover, a recently published study using skin prick tests for eight allergens in a young adult population in the State of São Paulo presented an atopy prevalence of 52%.5
It was seen that there were fewer smokers among the Brazilian cleaning workers than among the European workers26 (23% vs 50%, respectively). This probably contributed towards the lower rate of chronic bronchitis (3%) than among the European workers (7%).26 However, this difference may be partially explained by the definition of chronic bronchitis used in our study, which was the presence of productive cough in the morning for at least three months a year, for two consecutive years. This differed from the definition used in the above-mentioned study (productive cough on most days for at least three months a year).26 Nonetheless, even after excluding the criterion of two consecutive years, the prevalence remained lower.
We were unable to identify any differences between the frequencies of product use or tasks performed and the respiratory health effects (table 2). Perhaps this can be attributed to low power of statistical analysis for the categorical variables, which would therefore reflect an error in planning for the study. It may also be attributed to high variability between the locations and between the products used and cleaning tasks performed, and also to the low educational level of this workforce and a scarcity of information on the products and risks. We evaluated subcontracted workers from the southern region of the City of São Paulo and selected types of industrial/commercial enterprises. The sample was drawn from an eligible population of 5051 individuals. We did not have demographic and health characteristics from the remainder of the eligible population to compare with the sample. These criteria did not cause any bias in our results because it was a proportional sample. The majority of the eligible population consisted of subcontracted workers; there were no large differences between different parts of the metropolitan area, in terms of outdoor air pollutants. Activities that might have suffered from other interfering pollutants (such as hospitals, industrial plants and public parks) were excluded. As in most occupational studies, the main limitation to this study was the exposure assessment. Objective estimates are critical limitations, because cleaning tasks, workplaces (mobile work) and products are changeable during the workers’ routine, with intermittent exposure. It is extremely difficult to measure accidental peak exposures that are unpredictable and transient.36 In the absence of a control group, other studies have adopted office occupations as a reference group.6,9,10,26 Given that we could not match our sample with office workers, we compared internal prevalences according to different exposure levels (quartiles). Nevertheless, this reference group did provide the advantage of standardising other variables. We were unable to reduce potential confounding factors such as non-professional uses of cleaning products, living conditions, respiratory infections, dietary factors, environmental pollution and others. Unfortunately, such factors seem to be an inherent limitation to elucidating multifactorial determinants of disease.
Our findings add to other recently published studies that have given evidence of airway risks associated with the use of cleaning products. More detailed studies are necessary for characterising cleaning exposures and health effects, including analyses on building characteristics (carpet area, air conditioning and natural ventilation, among others). It is also important to know the timing between new-onset exposures and new-onset symptoms. We emphasise the need for cleaning product manufacturers to develop appropriate hazard labelling and safety precautions. Moreover, cleaning companies should provide workers with specific training on potential risks and implement preventive steps to minimise hazardous exposure, all within a comprehensive education programme emphasising the notion that cleanliness is next to healthiness.
Main messages
-
Approximately a third of asthma and a quarter of rhinitis cases among non-domestic cleaning workers may be related to occupation.
-
Asthma and/or rhinitis symptoms in non-domestic cleaning workers have a relation with length of exposure.
-
More than half of non-domestic cleaning workers relate airway symptoms to their work, and the agents most commonly related to these symptoms are chlorine and dust.
Policy implications
-
Cleaning workers are at risk of contracting work-related asthma and/or rhinitis, and this increases with exposure duration. The respiratory health surveillance for these workers needs to be reinforced.
-
Greater emphasis should be placed on interventions aimed at substituting the use of chlorine and encouraging more judicious use of this irritant in cleaning activities. Comprehensive educational activities should be adopted with the aim of controlling excessive use of cleaning products.
-
Further research on cleaning-related asthma should take into consideration possible irritant-induced asthma from repeated exposure to low-dose irritant cleaning chemicals.
Acknowledgments
The study was sponsored by FUNDACENTRO, Ministry of Labour and Employment, São Paulo, SP, Brazil. We thank the Cleaning Service Workers’ Union (SIEMACO) for contributing with the workplace database and workers’ registrations. The authors are grateful for the valuable comments and suggestions of the reviewers, which enriched the paper.
REFERENCES
Footnotes
-
Published Online First 15 February 2007
-
Competing interests: None declared.