Article Text

Abstract
The effect of acute and long-term exposures to outdoor particulate air pollution on lung function in healthy adults is not well established. The objective of this study was to conduct a systematic literature review and meta-analysis of studies that assessed the relationship of outdoor particulate air pollution and lung function in healthy adults. Studies that contained data on outdoor air particulate matter levels (PM10 or PM2.5) and forced expiratory volume in 1 s (FEV1) in healthy adults were eligible for inclusion. Effect estimates, in relation to long-term and acute exposures, were quantified separately using random effects models. A total of 27 effect estimates from 23 studies were included in this review. Acute exposures were typically assessed with PM2.5, while long-term exposures were predominantly represented by PM10. A 10 µg/m3 increase in short-term PM2.5 exposure (days) was associated with a −7.02 mL (95% CI −11.75 to –2.29) change in FEV1. A 10 µg/m3 difference in long-term PM10 exposure was associated with a −8.72 mL (95% CI −15.39 to –2.07) annual change in FEV1 and an absolute difference in FEV1 of −71.36 mL (95% CI −134.47 to –8.24). This study provides evidence that acute and long-term exposure to outdoor particulate air pollution are associated with decreased FEV1 in healthy adults. Residual confounding from other risk factors, such as smoking, may explain some of the effect for long-term exposures. More studies are required to determine the relationship of long-term exposure to PM2.5 and short-term exposure to PM10, which may have different biologic mechanisms.
- outdoor air pollution
- healthy adults
- spirometry
- lung function
- fev1
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Exposure to outdoor particulate air pollution has been associated with decreased lung function in patients with chronic obstructive pulmonary disease, but the relationship among healthy adults is less clear.
What are the new findings?
This meta-analysis shows that both acute and long-term exposure to outdoor particulate air pollution is significantly associated with decreased forced expiratory volume in 1 s (FEV1) in healthy adults.
Residual confounding from other factors, such as smoking, may explain some of this association for long-term studies.
How might this impact on policy or clinical practice in the foreseeable future?
Quantification of the adverse effects of air pollution on FEV1 in healthy adults may guide public awareness initiatives and air quality guidelines.
Introduction
Particulate matter is a complex mixture of liquid droplets and extremely small particles composed of both organic and inorganic compounds. Sources of ambient particulate matter include automobile emissions, construction sites, smokestacks, power plants, fires and brush burning. The composition of particulate matter to which an individual or population is exposed is dependent on the source or sources of exposure. Given the difficulty in determining the distinct compositional nature of the exposure, outdoor air pollution is most commonly measured by mass concentration of particulate matter with aerodynamic diameter less than 10 µm (PM10) or 2.5 µm (PM2.5), which each have distinct biological mechanisms. Animal models have found that PM10 can penetrate the conducting airways of the respiratory system, while PM2.5 can deposit into the gas-exchanging regions of the lung.1
In humans, both PM10 and PM2.5 have been shown to adversely affect the respiratory system and have also been shown to be associated with increases in all-cause mortality,2 3 lung cancer,3 stroke4 and hospital admissions for chronic obstructive pulmonary disease (COPD) and asthma.2 5 There is increasing evidence that particulate air pollution exposure is linked to new-onset pulmonary and cardiovascular disease in previously healthy individuals.6 Geographically, there is a large variation in the levels of particulate matter. According to the WHO Global Ambient Air Quality Database, annual mean concentrations of PM10 and PM2.5 between 2015 and 2016 were relatively low in large North American and European cities, such as Toronto (16 µg/m3 and 9 µg/m3), New York (14 µg/m3 and 7 µg/m3) and London (21 µg/m3 and 11 µg/m3). In comparison, levels were considerably higher in large cities of India, China and the Eastern Mediterranean, such as New Delhi (292 µg/m3 and 143 µg/m3), Beijing (92 µg/m3 and 73 µg/m3) and Cairo (284 µg/m3 and 117 µg/m3), respectively.7
Long-term exposures to ambient particulate air pollution tend to represent average trends over time, while acute exposures may represent larger fluctuations over a short period, and these may have different consequences in terms of health outcomes. The effects of air pollution on lung function can be quantified by measuring changes in spirometric lung parameters such as the forced expiratory volume in 1 s (FEV1). Reduced FEV1 has been shown to be associated with stroke, cardiovascular mortality and all-cause mortality, making it an important endpoint to study. Studies examining the effect of acute exposures to air pollution on lung function use temporal variation in air pollution (same location over a number of days), while studies examining the effect of long-term exposures utilise spatial variation (different locations over months to years). Lung function in relation to air pollution can be assessed either by comparing changes in FEV1 over a specified time period within subjects or by comparing absolute FEV1 at a single time point between subjects.
While the relationship between exposure to particulate air pollution and lung function in individuals with COPD has been summarised,8 the relationship among healthy individuals is not fully understood. A large multicentric cohort study in Western Europe assessed the effect of long-term exposure to particulate air pollution on lung function in healthy adults and adults with asthma (European Study of Cohorts for Air Pollution Effects (ESCAPE) study).9 In this study, they found inverse associations between long-term air pollution and baseline FEV1 but did not detect a significant association between long-term exposure to air pollution and change in FEV1 over time. Despite this large cohort study, there has not been a meta-analysis on the effect of acute or long-term exposure to outdoor particulate air pollution.
Improved understanding of the impact of air pollution on lung function may have considerable clinical relevance, as decreases in FEV1 have been associated with increases in mortality from lung cancer, cardiovascular disease and all-causes,10 11 as well as decreases in quality of life.12 The objective of this study was to quantify the effect of both acute exposure and long-term average exposure to outdoor particulate air pollution on the lung function of healthy adults throughout the world by performing a comprehensive systematic review and meta-analysis.
Materials and methods
Search strategies and selection
A systematic literature search of English language publications of adults greater than 18 years of age was conducted by SE using Embase, MEDLINE, Cochrane Library and citation review from 1991 to August 2018. The MeSH and Emtree terms used for each of the database searches and details of our full search strategy are provided in online supplementary table 1. SE and DEO identified additional studies by inspecting references of the included studies and literature reviews. Contact with authors was not conducted. Acquired literature was reviewed, and inclusion was independently assessed by SE and DEO. Agreement between the two reviewers was quantified using per cent agreement and a kappa statistic. Disagreements were resolved by discussion. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist was followed to report this systematic review and the meta-analysis findings.
Supplementary file 1
Inclusion and exclusion criteria
Initial inclusion criteria for articles were: (1) original studies; (2) outdoor particulate air pollution as exposure; (3) PM10 or PM2.5 as particulate air pollution metric; (4) lung function measure was FEV1; and (5) healthy populations (defined as prevalence of lung disease <10%). We formulated strict exclusion criteria for articles. These included: (1) populations with a diagnosis of COPD, asthma or other respiratory disease; (2) did not consider PM10 or PM2.5; and (3) effect estimate not reported or could not be derived from the information provided.
Data extraction
Relevant information from included studies was extracted by SE. These included study design, time-period, location, age of subjects, pollution parameter measured, resolution of air pollution measurement, statistical analysis and confounders adjusted for. All effect measures were transformed to per 10 µg/m3 increase in particulate matter, assuming a linear relationship between the concentration of particulate matter and lung function. For studies that presented results in exposure categories, a continuous effect per 10 µg/m3 of particulate matter was obtained by using the midpoints of the categories of particulate air pollution and performing a weighted linear regression.13 If a study presented a CI, the corresponding SE was calculated as (upper CI−lower CI)/([xn−x0]*3.92), where CI is confidence interval, xn denotes exposure at group n level and x0 denotes exposure at reference group. The SE for the effect estimate was computed using the approach described in Greenland and Longnecker.14 If a study reported only an effect estimate and a p value, we used the Bland and Altman method to obtain a CI and corresponding SE.15 Studies assessing the effect of acute exposure to air pollution often reported different time periods (lag of 0, 1 or 2 days and so on). Whenever possible, we recorded the effect noted at 1 day after exposure. For studies that presented effect estimates as change in per cent predicted FEV1, an average predicted FEV1 for the sample was estimated using the European Respiratory Society reference calculator16 based on average age, sex, height and ethnicity of the study participants. The per cent of the predicted FEV1 was used as the baseline to quantify the absolute change in FEV1 in millilitres.
Meta-analysis
A meta-analysis was performed if there were three or more studies that had the same study design and air pollution measurement. Study designs were classified as longitudinal (prospective cohort and panel studies) or cross-sectional, and air pollution measures were either PM10 or PM2.5. Effect estimates per 10 µg/m3 were combined to calculate summary effect estimates using generic inverse variance method assuming a random effects model. Heterogeneity among studies was statistically investigated with the Q-test and the use of the I2 statistic.17 To assess publication bias, we visually reviewed funnel plots and employed both Egger’s weighted linear regression18 and Begg’s rank correlation tests.19 In the presence of statistically significant publication bias the trim and fill approach was employed to obtain an unbiased summary effect estimate.20 Given that the Begg’s and Egger’s tests are underpowered in meta-analyses with few studies,21 in the presence of statistically insignificant publication bias, we also employed the trim and fill approach to ensure the validity of our results. All analyses were performed using the R computing framework (http://www.r-project.org).
Study quality assessment and sensitivity analyses
For studies assessing the relationship between acute exposure to outdoor particulate matter and FEV1, we conducted subgroup analyses by the type of air pollution measurement (fixed site vs personal sampler) and activity (exercise vs other). For studies assessing the relationship of long-term exposure to air pollution and FEV1, we conducted subgroup analyses by the time and spatial resolution of the air pollution measurement, as well as by adequate control for confounding. For change in FEV1, time resolution was defined as measurement for a period less than a year and measurement for a period of a year or greater. For absolute FEV1, time resolution was defined as measurement for a year and measurement for a period greater than a year. Spatial resolution was defined as less than 1 km by 1 km resolution or interpolation from fixed site monitors and greater than 1 km by 1 km resolution. Studies were considered to have adequately controlled for confounding if they adjusted for age, sex, smoking, body mass index and a measure of socioeconomic status. Given that smoking is a particularly important confounder in this relationship, we also conducted a subgroup analysis by studies that included only non-smokers and studies that included both smokers and non-smokers.
The ESCAPE study includes a heterogeneous set of cohorts with respect to prevalence of lung disease. Fourteen per cent of the individuals from the ESCAPE study had asthma, but three of the five included cohorts had a prevalence less than 10%. When an analysis of long-term exposure to air pollution did not include more than one of these three cohorts (from a previous publication), we conducted a sensitivity analysis including the result of the entire ESCAPE study to test the validity of our results.
Results
Search findings and study characteristics
In total, 336 studies were identified in the initial MEDLINE and Embase search, while no studies were identified in the Cochrane database (figure 1). Forty-four studies from the database search and 16 additional studies identified from reference lists and secondary sources underwent full-text review. After full-text screening, 23 studies were included in this review. Of the 23 studies included, 22 were identified through the online search,22–43 and one study was identified from additional sources.44 The primary reason for exclusion was a study population that included a considerable portion (greater than 10%) of individuals with pre-existing respiratory diseases (asthma or COPD). Secondary reasons for exclusion included a lack of measurement of particulate matter (PM2.5 or PM10) or FEV1. Two studies26 43 were not included in a meta-analysis, because they contained too many differences to be pooled with other studies (less than three studies that had the same air pollution measurement, type of exposure and study design). The results of these studies are described. There was good agreement between the two reviewers for the full-text review. The percent agreement and kappa statistics were 88.3% and 0.72, respectively.
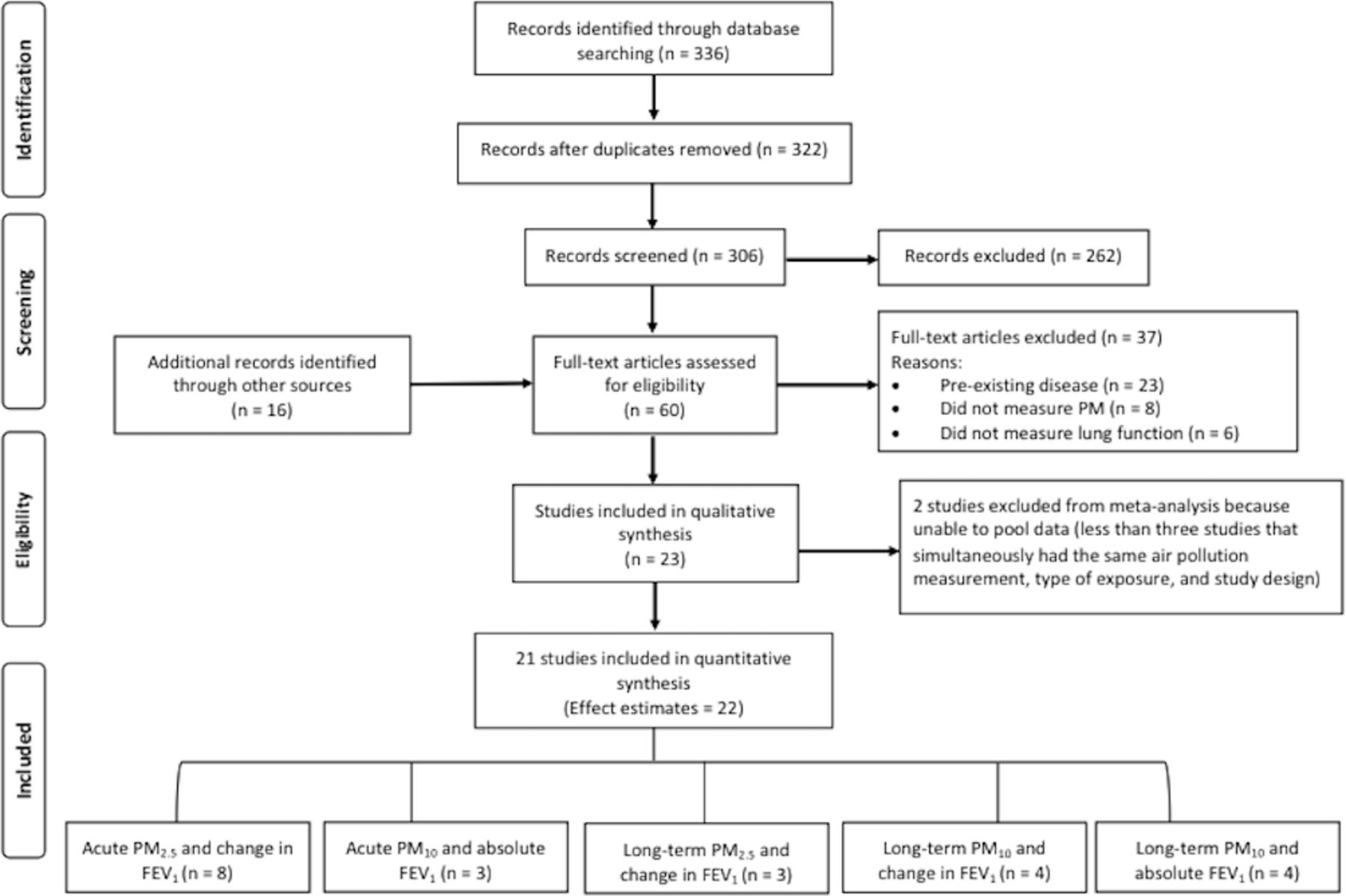
Flow diagram of the selection procedure of studies assessing the relationship of acute and long-term exposure to outdoor particulate air pollution and FEV1 in healthy adults. Description: a PRISMA flow diagram that details the inclusion and exclusion of studies considered for this systematic review. FEV1, forced expiratory volume in 1 s; PM2.5, particulate matter with aerodynamic diameter less than 2.5 µm; PM10, particulate matter with aerodynamic diameter less than 10 µm; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The association between acute exposure to outdoor particulate air pollution and lung function in healthy adults
Characteristics of the 13 studies investigating the relationship of acute exposure to outdoor particulate air pollution and lung function in healthy adults in presented in table 1.25 26 30 32–35 37–40 43 44 Data from a total of 15 766 individuals from eight different countries were examined in these reports. Of the included studies, five were conducted in North America, three in China and one study was conducted in each of Brazil, India, the Netherlands and Israel. The majority of the included studies assessed the change in FEV1 associated with acute exposure to air pollution (n=9) and used PM2.5 as the exposure metric (n=10). From available data, 5.6% of participants were current smokers, and 3.1% had pre-existing respiratory conditions (primarily asthma or wheeze).
Characteristics of studies investigating the association of acute exposure to outdoor particulate air pollution and FEV1 in healthy adults (n=13)
Eight studies assessed the relationship between acute exposure to PM2.5 and change in FEV1.30 32–35 37 44 A random effects model yielded a pooled estimate of daily change in FEV1 of −7.02 (95% CI −11.75 to −2.29) associated with an acute exposure to 10 µg/m3 change in PM2.5 (figure 2A). There was moderate heterogeneity (I2=49.1%) among studies included in this analysis, and there was statistical evidence of publication bias (Egger’s regression test; p=0.06). The trim and fill method identified two unpublished studies and yielded an unbiased estimate of a change in FEV1 of −6.13 (95% CI −10.78 to −1.48) associated with an acute exposure to 10 µg/m3 change in PM2.5. One study assessed the relationship between acute exposure to PM10 and observed a significant change in FEV1 of −15.8 mL (95% CI −21.9 to −9.6) per 10 µg/m3 increase in PM2.5.43
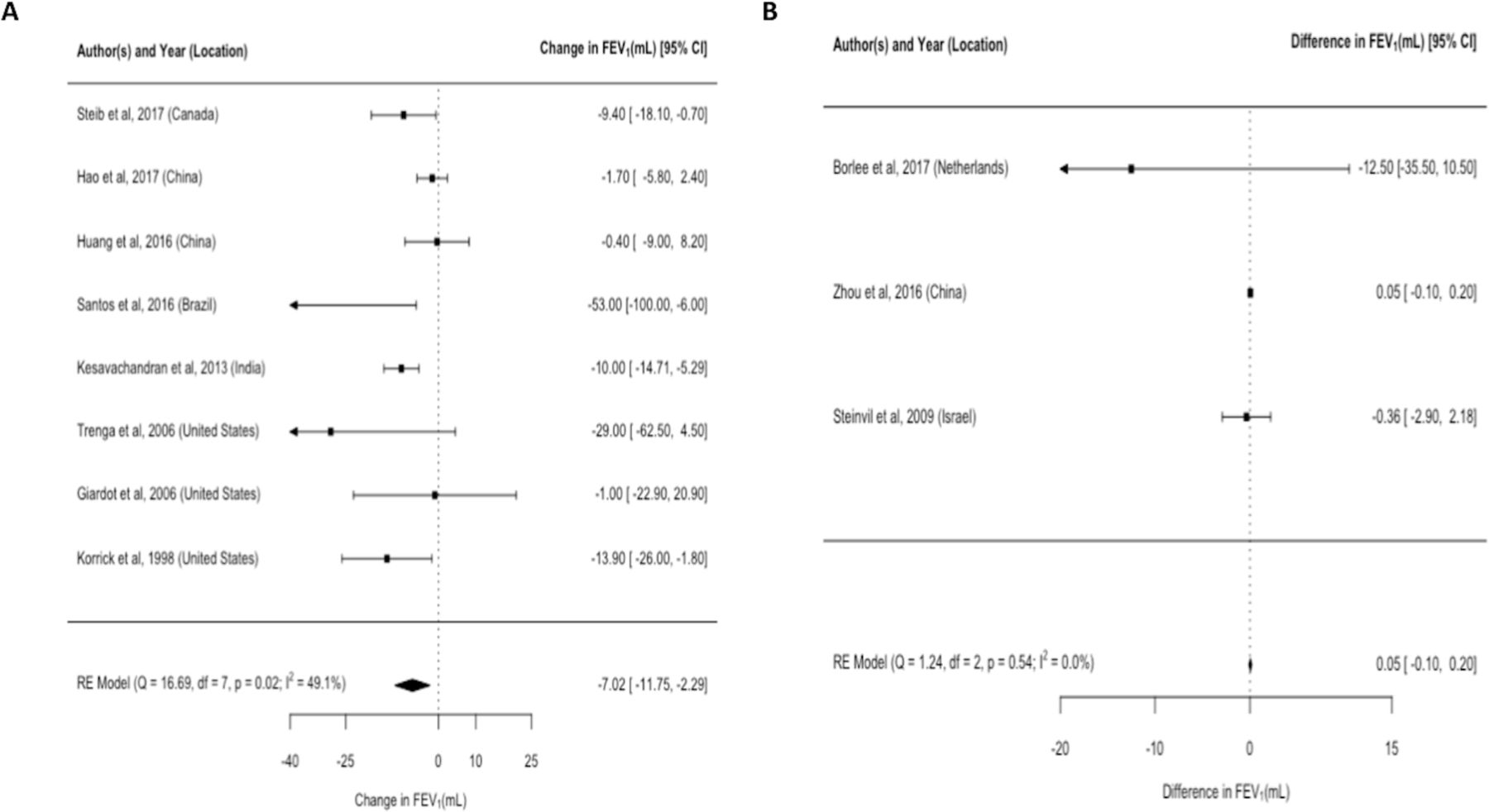
The effect of acute exposure to PM2.5 and FEV1 in healthy adults. Description: panel A displays a forest plot of study-specific and pooled change in FEV1 associated with an increase in acute exposure to PM2.5 of 10 µg/m3. Panel B displays a forest plot of study-specific and pooled difference in FEV1 associated with greater acute exposure to PM10 of 10 µg/m3. FEV1, forced expiratory volume in 1 s; PM2.5, particulate matter with aerodynamic diameter less than 2.5 µm; PM10, particulate matter with aerodynamic diameter less than 10 µm; RE, random effect.
Three studies assessed the relationship between acute exposure to PM10 and absolute difference in FEV1.25 38 40 A random effects model yielded a pooled estimate of absolute difference in FEV1 of 0.05 mL (95% CI −0.10 to 0.20) associated with 10 µg/m3 increase in exposure to PM10 (figure 2B). There was no heterogeneity (I2=0.0%) across the included studies, and there was no statistical evidence of publication bias (Egger’s regression test; p=0.32). Two studies assessed the relationship between acute exposure to PM2.5 and observed a nonsignificant absolute differences in FEV1 of 0.13 mL (95% CI −0.26 to 0.51)40 and −40.29 mL (95% CI −71.89 to 8.50)26 per 10 µg/m3 increase in exposure to PM2.5.
The association between long-term exposure to outdoor particulate air pollution and lung function in healthy adults
Characteristics of the 10 studies investigating the relationship of long-term exposure to outdoor particulate air pollution and lung function in healthy adults are presented in table 2.22–24 27–29 31 36 41 42 A total of 64 301 individuals from 13 different countries were examined in these reports. These studies were primarily conducted in Europe (n=5) and the USA (n=3), while the remaining studies were conducted in India and Japan, respectively. Six studies assessed the relationship of air pollution with change in FEV1, while six examined the difference in FEV1 between individuals living at different levels of air pollution (two studies31 34 examined both relationships). Among studies assessing change in FEV1, the majority used PM10 (n=4) as the air pollution metric, while all except one study assessing differences in FEV1 used PM10 as the air pollution metric. From available data, 21.5% of participants were current smokers, and 7.7% had pre-existing respiratory conditions (primarily asthma or wheeze).
Characteristics of studies investigating the association of long-term exposure to outdoor particulate air pollution and FEV1 in healthy adults (n=10)
Four studies assessed the relationship between long-term exposure to PM10 and annual change in FEV1.24 27 28 42 A random effects model yielded a pooled estimate of annual change in FEV1 associated with a 10 µg/m3 difference in PM10 of −8.72 mL (95% CI −15.39 to –2.07; figure 3A). Among this literature base, there was high heterogeneity (I2=78.2%), and there was statistical evidence of publication bias (Egger’s regression test; p=0.04). The trim and fill method identified one unpublished study and yielded an unbiased estimate of an annual change in FEV1 of −7.41 mL (95% CI −13.67 to –1.15) associated with a 10 µg/m3 difference in PM10.

{kind=link}
{kind=link}
{kind=link}
The effect of long-term exposure to PM10 and FEV1 in healthy adults. Description: panel A displays a forest plot of study-specific and pooled change in FEV1 associated with an increase in long-term exposure to PM10 of 10 µg/m3. Panel B displays a forest plot of study-specific and pooled difference in FEV1 associated with greater long-term exposure to PM10 of 10 µg/m3. *Men-only estimate; **women-only estimate. FEV1, forced expiratory volume in 1 s; PM2.5, particulate matter with aerodynamic diameter less than 2.5 µm; PM10, particulate matter with aerodynamic diameter less than 10 µm.
Three studies assessed the relationship between long-term exposure to PM2.5 and annual change in FEV1.24 31 36 A random effects model yielded a pooled estimate of annual change in FEV1 associated with 10 µg/m3 difference in PM2.5 of 0.36 mL (95% CI −0.27 to 0.98).24 31 36 There was low heterogeneity among these studies (I2=8.9%) and evidence of publication bias. The trim and fill method identified two unpublished studies and yielded an unbiased estimate of an annual change in FEV1 of 0.45 mL (95% CI −0.31 to 1.19) associated with a 10 µg/m3 difference in PM2.5.
Four studies assessed the relationship between long-term exposure to PM10 and absolute difference in FEV1.22 23 29 41 A random effects model yielded a pooled estimate of absolute difference in FEV1 of −70.4 mL (95% CI −136.15 to –4.65) associated with 10 µg/m3 difference to PM10 (figure 2B). There was a high degree of heterogeneity (I2=93.0%) across the included studies, and there was no statistical evidence of publication bias (Egger’s regression test; p=0.54).
Two studies assessed the relationship between long-term exposure to PM2.5 and absolute FEV1. One study observed a significant absolute difference in FEV1 of −67 mL (95% CI −133.0 to –15.0) per 10 µg/m3 difference in PM2.5,36 while another study observed a significant absolute difference in FEV1 of 470.5 mL (95% CI 153.8 to 787.2) for men and a non-significant difference of 95.6 mL (95% CI −31.3 to 222.5) for women per 10 µg/m3 difference in PM2.5.31
Study quality assessment and sensitivity analyses
Subgroup and sensitivity analyses for each meta-analysis is presented in online supplementary table 2. Among studies assessing the relationship between acute exposure to PM2.5 and change in FEV1, the air pollution measurement, activity, control for confounding and smoking status of the population were not significant sources of heterogeneity. Among studies assessing the relationship of long-term exposure to PM10 and change in FEV1, the length of measurement and smoking status of the population were significant sources of heterogeneity. Among studies assessing the relationship of long-term exposure to PM10 and absolute FEV1, spatial resolution and smoking status of the population were significant sources of heterogeneity.
Supplementary file 1
Discussion
This study contains, to our knowledge, the first meta-analyses assessing the effects of outdoor particulate air pollution on FEV1 in healthy adults including studies throughout the world. We examined the effect of both acute and long-term exposure to particulate air pollution on absolute lung function and changes in lung function among healthy adults. We found that increasing levels of average PM2.5 were associated with a statistically significant change in FEV1 (−7.02 mL/day per 10 µg/m3 increase in PM2.5). We also observed that increasing levels of average PM10 were associated with statistically significant yearly changes in FEV1 (−8.73 mL/year per 10 µg/m3 difference in PM10) and with lower absolute FEV1 (−71.36 mL per 10 µg/m3 in PM10).
Publication bias was present in this body of literature; however, correction for this bias with the trim and fill method did not considerably change the results. In sensitivity analyses according to study quality (control for confounding and air pollution measurement), we observed significant differences in results based on time and spatial resolution of the air pollution measurement, as well as the smoking status of the study population. Studies with better resolution tended to have smaller effects but were still statistically significant. Studies of long-term exposure to air pollution that included both smokers and non-smokers tended to have larger effects, suggesting that residual confounding from smoking is present in this literature. However, when restricting to studies that only included non-smokers, long-term exposure to PM10 was still associated with a significant reduction in FEV1. Results for acute exposures were stronger for studies that involved exercise, suggesting that physical activity may amplify the effect of air pollution on acute lung function. However, these subgroup analyses were based on a small number of studies and should therefore be interpreted with caution.
Our findings are similar to those seen in the ESCAPE study.9 Among cross-sectional studies, they found that differences of average PM10 per 10 µg/m3 were associated with a statistically significantly lower baseline FEV1 of 44.56 mL. The larger effect size of −71.36 mL in our meta-analysis could be partially attributed to residual confounding, given that the ESCAPE study had standardised measurements across the included studies, while we were limited by heterogeneity in this regard. While the ESCAPE study did not find a statistically significant effect of PM10 on yearly change in FEV1, we found a statistically significant yearly decrease in FEV1 (8.72 mL). Differences between the study populations may explain the difference in effects between the two meta-analyses, as the ESCAPE study contained twice as many adults with asthma and 21% more smokers. Similar to the ESCAPE study, we did not find a significant reduction in FEV1 with long-term exposure to PM2.5. However, only one study adequately controlled for confounding. Our sensitivity analysis including the result of the ESCAPE study yielded similar results.
The large difference observed between the change in FEV1 and absolute differences in long-term studies could be a result of a number of factors. First, studies assessing the effect on lung function at one time point are capturing the effect of air pollution over a longer period of time, assuming that individuals have been residing in those areas for a long period. In contrast, studies assessing changes in lung function are only capturing the effect of air pollution over a year as the baseline spirometry controls for the effect of all previous exposure to air pollution. Second, given the longer exposure period for studies assessing absolute difference in lung function, the results of these studies are more susceptible to residual confounding from factors related to lung function, such as smoking and obesity.
Decreased lung function from long-term exposure to ambient particulate pollution has a number of potential adverse consequences for healthy adults. A reduced FEV1 is associated with increased rates of stroke,45 cardiovascular mortality10 and all-cause mortality.11 The health implications of acute exposures to ambient particulate air pollution have been described in vulnerable populations but are less clear among healthy adults. Daily fluctuations in particulate air pollution have been associated with increases in admissions for asthma,46 COPD and pneumonia in the elderly.47 Similar to the effect of an acute respiratory tract infection on smokers with and without COPD,48 the effects of acute exposures to particulate air pollution tend to be smaller compared with the effects of exposure over a longer time period. This may be due to a cumulative effect of consistent exposure to high levels of air pollution. It is unclear, however, if repeated acute exposure to high levels of air pollution can have long-term health implications. Future longitudinal studies are required to clarify this possibility among healthy individuals.
The effect sizes observed appear to be relatively modest. However, they represent the effect with a change in PM2.5 or PM10 of 10 µg/m3. In North America and many European countries, levels remain low, and there is not significant fluctuation. However, in developing countries, the pollution levels can vary quite dramatically. In a Chinese study, daily PM2.5 levels fluctuated by nearly 100 µg/m3 in under 1 week.32 This could imply a 10-fold increase in the effect size, assuming a linear relationship which, in turn, could lead to a much larger and clinically significant effect on lung function. A change in FEV1 of 100 mL is often considered to be a minimal clinically important difference in respiratory trials.49
A limitation of our meta-analysis was the small number of studies within each subgroup. Older studies tended to use PM10 as their particulate pollution measure, whereas newer studies more commonly use PM2.5 as it is now widely held that it contains the fraction of PM that is more harmful to human health.50 Because of this change in measurement, it is difficult to compare newer studies to older studies. In addition, we were unable to stratify our analyses by geography, where larger differences in the level and composition of air pollution could be present and may have different effects on lung function.
Despite these limitations, our study had a number of strengths. It is the first to characterise the effects of air pollution on lung function across multiple continents and is to our knowledge the first meta-analysis to demonstrate a significant decrease in lung function with both long-term and acute exposures in healthy adults. We reduced heterogeneity in our analyses by strictly separating studies by a number of factors, including study design, time course and air pollution parameter. We also used a consistent lag time when selecting data from studies to reduce potential bias. We attempted to address the issue of confounding by performing subgroup analyses and the issue of residual confounding by smoking through sensitivity analyses that restricted to only studies of non-smokers.
Conclusion
In summary, our results demonstrate that both acute and long-term exposure to outdoor particulate air pollution are associated with reductions in FEV1among healthy adults. Further research is required to better quantify and compare the effects of air pollution across populations and exposure metrics. Future studies should stratify by high and low pollution levels to determine if baseline pollution level has an impact on the magnitude of association of exposure to particulate air pollution and lung function.
Acknowledgments
DO is supported by a Queen Elizabeth II Scholarship and an Empire Life Fellowship.
References
Footnotes
Contributors SE, DEO and DL contributed to the study design; SE conducted the literature search and abstract screening; SE and DEO carried out the full-text review; DEO conducted the statistical analyses; WK provided guidance of the statistical analyses and revised the manuscript; SE, DEO and DL wrote and revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests DL reports personal fees from Public Service Occupational Health Program Regions and Programs Bureau Health Canada/Government of Canada, and honoraria from the Astra Zeneca PRECISION Program during the conduct of the study; other (all paid directly to Queen’s University) from: grant from Astra Zeneca, grant from GlaxoSmithKlein, grant from Hoffman LaRoche Ltd., grant from Novartis, grant and other from Ontario Lung Association, grant from Government of Ontario’s Innovation Fund, grant from Allergen NCE, grant from Janssen, grant from Canadian Institutes of Health Research, outside the submitted work
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.