Article Text

Abstract
Context More than 400 000 workers annually receive a measurable radiation dose and may be at increased risk of radiation-induced leukaemia. It is unclear whether leukaemia risk is elevated with protracted, low-dose exposure.
Objective We conducted a meta-analysis examining the relationship between protracted low-dose ionising radiation exposure and leukaemia.
Data sources Reviews by the National Academies and United Nations provided a summary of informative studies published before 2005. PubMed and Embase databases were searched for additional occupational and environmental studies published between 2005 and 2009.
Study selection We selected 23 studies that: (1) examined the association between protracted exposures to ionising radiation and leukaemia excluding chronic lymphocytic subtype; (2) were a cohort or nested case–control design without major bias; (3) reported quantitative estimates of exposure; and (4) conducted exposure–response analyses using relative or excess RR per unit exposure.
Methods Studies were further screened to reduce information overlap. Random effects models were developed to summarise between-study variance and obtain an aggregate estimate of the excess RR at 100 mGy. Publication bias was assessed by trim and fill and Rosenthal's file drawer methods.
Results We found an ERR at 100 mGy of 0.19 (95% CI 0.07 to 0.32) by modelling results from 10 studies and adjusting for publication bias. Between-study variance was not evident (p=0.99).
Conclusions Protracted exposure to low-dose gamma radiation is significantly associated with leukaemia. Our estimate agreed well with the leukaemia risk observed among exposed adults in the Life Span Study (LSS) of atomic bomb survivors, providing increased confidence in the current understanding of leukaemia risk from ionising radiation. However, unlike the estimates obtained from the LSS, our model provides a precise, quantitative summary of the direct estimates of excess risk from studies of protracted radiation exposures.
- Epidemiology
- leukaemia
- radiation
- health and safety
- meta-analysis
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Introduction
What this paper adds
Each year millions of people incur low doses of protracted ionising radiation as a condition of either employment or medical treatment.
It is unclear whether cancer risks estimated in this population reflect actual risks given that current models are based principally on the acutely exposed cohort of Japanese atomic bomb survivors.
A meta-analysis was conducted to synthesise existing information in 23 studies of leukaemia risk from protracted ionising radiation exposure.
Although information on leukaemia risks varied, a synthesis of this information revealed a significant association between leukaemia (excluding CLL) and protracted exposure to low-dose ionising radiation.
Occupational and environmental studies of low-dose ionising radiation exposure may individually lack the precision necessary for risk estimation; however, information from meta-analysis of these studies may be useful in elucidating risks and ultimately play an important role in the development of future protection standards.
Each year, approximately 4 million US patients are exposed to low-dose ionising radiation through medical diagnostic procedures.1 Moreover, according to estimates by the United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR), over 11 million workers worldwide are exposed to ionising radiation each year.2 Epidemiological evidence unequivocally establishes ionising radiation as a human carcinogen3 4; thus, safeguards have been established to mitigate cancer risks in exposed populations. For over 50 years, risk models forming the basis of radiation protection standards have been based almost exclusively on the Life Span Study (LSS) cohort of Japanese atomic bomb survivors. It is unclear whether cancer risks estimated from this population reflect actual risks in populations exposed to low-dose, protracted ionising radiation.
Leukaemia, excluding the chronic lymphocytic subtype (CLL), is considered to be among the cancers most susceptible to induction by ionising radiation exposure5; thus, leukaemia risk in environmentally and occupationally exposed populations has been studied extensively. Therefore, our goal was to synthesise available information from observational studies of these populations to obtain an aggregate estimate of the excess RR for persons receiving a whole-body absorbed dose of 100 mGy.
Aggregate risks are typically estimated using pooled or meta-analytical approaches. In the former case, individual-level data are combined across studies to estimate the effect size. In the latter, risk estimates from individual studies are compared and then combined into an aggregate estimate. While both methods can provide an efficient summary estimate, it is difficult to control for differences in data quality across subpopulations in pooled studies. Moreover, obtaining raw data from multiple studies, each with its own set of data protection requirements, can be daunting. Thus, we conducted a meta-analysis of leukaemia risk from ionising radiation using published data.
The study population was restricted to adults exposed to low-dose ionising radiation in occupational and environmental settings. Studies of medical therapy patients and childhood leukaemias in populations near nuclear facilities were excluded. We also limited our synthesis to populations exposed primarily to low linear energy transfer (LET) radiations, and thus studies of radon-exposed populations, uranium miners and millers, and aircraft crews were excluded.
Methods
Search
A review by the National Academies provided a comprehensive summary of informative studies published prior to 2005.6 We also reviewed the latest report by UNSCEAR for relevant publications.7 To add to existing information, two researchers independently and systematically searched the PubMed and Excerpta Medica (Embase) databases for additional studies published between January 2005 and March 2010. The search was completed using an English language restriction. The key terms “ionising radiation”, “epidemiology”, “dose reconstruction”, “leukemia” and “leukaemia” were used in the initial searches, which were later refined using additional terms such as “cancer incidence”, “cancer mortality”, “Mayak”, “Techa River”, “Chernobyl”, “Chornobyl”, “liquidators”, “radiological technologist”, “nuclear industry”, “occupational radiation” and “x-ray”. Abstracts were reviewed to determine the applicability of articles under consideration. After consolidating the results of both searches, the published articles were independently evaluated for inclusion by each researcher. Citations within informative articles were then used to identify other informational sources.
Study selection
Criteria for identifying informative studies were adopted, with modification, from methods used by the National Research Council.6 For a study to be included in our analyses, it must: (1) examine the association between protracted human exposures to ionising radiation and leukaemia excluding CLL; (2) be a cohort or nested case–control design without major identifiable bias (eg, significant exposure misclassification or confounding by concomitant leukaemogen exposures); (3) use individualised quantitative estimates of absorbed dose, or dose equivalent, to the whole body or organ of interest (ie, active bone marrow); and (4) report exposure–response analyses in terms of excess RR per unit dose (D) whereby RR=1+ERR(D), or RR at a given exposure level using within-cohort comparison. The exposure term must be quantified in units of absorbed dose in gray (Gy), or derived protection quantities in sievert (Sv).8 9 We selected the effect size associated with low-LET external radiation exposures, if reported separately. In other cases, the differences between absorbed dose and the protection quantities were considered minimal due to the relatively high contribution of low-LET penetrating radiation to the total dose compared to other sources of radiation exposure.
Many radiation-exposed populations have been studied repeatedly and in pooled settings; therefore, we found numerous instances of overlapping information. Publications were thoroughly examined for redundancy. Overlapping studies were then vetted based on design, study coverage and relevancy. Studies with recent follow-up and dosimetry were preferred. When follow-up periods were relatively equal, cohort studies were preferred over case–control designs unless the case–control study offered marked improvement in dose reconstruction and control for confounding.
Statistical methods
Statistical analysis were conducted using the Mixed Procedure in SAS V. 9.210 and the Metafor Package in R.11 Effect size and precision estimates were abstracted from each study and used in hierarchical random effects models12 to obtain a pooled estimate,
Pooling was accomplished using a weighted average of individual study effect size estimates,
Both pooled and ‘stand-alone’ studies were available for meta-analysis. Given expected difficulties in minimising information overlap with varying combinations of studies, two general combination schemes were used, whereby model I preferred stand-alone studies while model II included pooled analyses. Sensitivity analyses employed the quantity DFFITS, defined as the difference between the effect size of the full model and the effect size from the fitted model with the ith study removed, divided by the standard error of the reduced model. Leave-one-out sensitivity analyses were used to judge single study influence in both models whereby the DFFITS statistic for each study was compared to a cut-off value (maxDFFITS).11 The cut-off values were defined as
Publication bias was assessed by funnel plot using Egger's regression16 and trim and fill methods.17 Rosenthal's ‘file drawer’ method was used to estimate the fail-safe N, which is the number of potentially unpublished null studies required for the overall effect to be non-significant at the 95% level (one-tailed).18 We considered publication bias to be extremely unlikely when fail-safe N>5k+10. Effect sizes were adjusted to account for publication bias using trim and fill methods by including the ‘missing’ studies in subsequent random effects models.
Results
Literature review
The BEIR VII Report provided 16 occupational studies that were potentially informative for our analysis.6 We examined another 55 studies published before 31 March 2010 (online figure 1). Of the combined total (n=71), 33 studies did not meet our inclusion criteria and 15 were superseded by other published information. The remaining 23 studies, hereafter referred to as ‘primary’, were found suitable for meta-analysis (table 1).
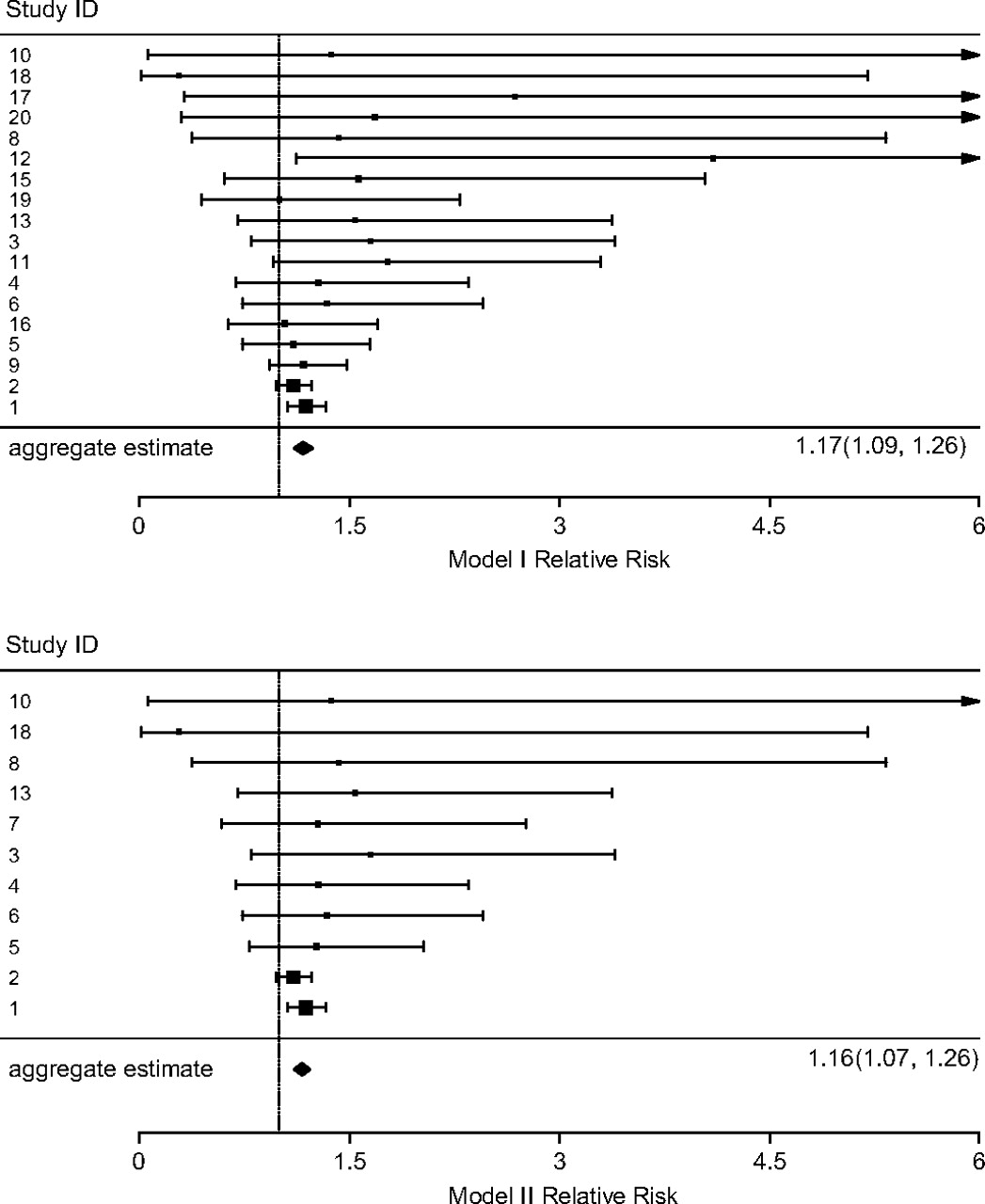
Forest plots of model I (top) and model II (bottom) random effects models estimating RR at 100 mGy. Dotted line references no effect (ie, RR=1). The effect point sizes (■) are drawn proportional to the inverse of the sampling variances. Lower bound of confidence intervals may differ from published values because of assumptions on standard errors.
Primary studies selected for meta-analysis
The primary studies were published between 1993 and 2009 and provided risk estimates for populations in occupational (n=20) and environmental settings (n=3). Of the environmental exposure studies, one examined the effects of exposures to elevated natural background radiation. The two remaining studies examined exposures from man-made sources. Occupational studies included cohorts from nuclear weapons facilities (n=6), the commercial power industry (n=6), clean-up and restoration activities (n=2), nuclear shipyards (n=2), or a combination of industry sectors (n=4).
Exposure distributions were highly skewed; the average cumulative exposure ranged from 5.6 to 810 mGy. Exposure information was obtained from personal monitoring data in most occupational settings, although monitoring may have been incomplete or highly uncertain in some studies.22 26 Personal monitoring data were not available for environmental studies; thus, doses were estimated using complex dosimetry systems.19 21 28
Most studies evaluated leukaemia mortality risk; however, five studies (study nos. 1, 4, 8, 10 and 21) reported leukaemia incidence. Twenty studies reported risk estimates from linear ERR models. The remaining three studies (nos. 1, 6 and 20) estimated the leukaemia RR at 100 mGy exposure in which the radiation effect was modelled as log-linear in dose. There were 19 retrospective cohort studies and four nested case–control designs. All selected study endpoints excluded contributions from CLL.
Assessment of overlap and combining studies
Of the 23 primary studies, 18 (IDs 1–5b, 6, 8–13, 15–20) were included in model I, and model II comprised 11 studies (IDs 1–5a, 6, 7b, 8, 10, 13, 18). Several studies were not completely independent; however, we were able to use combinations of study information in all models that did not overlap. Studies of particular importance and the steps taken to prevent duplicate information are discussed herein. Study no. 5 examined leukaemia mortality among nuclear workers from four US weapons facilities and a naval shipyard.23 Study no. 7 reports mortality in a cohort of approximately 400 000 nuclear workers from 15 different countries.25 Forty-seven leukaemia deaths among participants in study no. 5 were also included in study no. 7. Model II, combining both studies, was restricted to the full cohort of study no. 5 (ID 5a) and a subset of study no. 7 (ID 7b) that excluded US workers. Likewise, a subset of study no. 5 (ID 5b) was used to eliminate overlapping information on US weapons workers reported by study no. 11.
Many subpopulations included in study no. 7 were also individually examined in separate publications.27 33 35 37 38 In defining model I, we used stand-alone studies in preference to available subpopulation information published in study no. 7. Three studies (IDs 14, 16, 21) examined leukaemia risks among Canadian nuclear workers.32 34 39 These studies differed in cohort definition and outcomes measured, but study no. 16 best satisfied model I inclusion criteria.
Modelling results
The main statistical analyses are summarised in tables 2 and 3. Forest plots of both full models are shown in figure 1. The model I ERR at 100 mGy was significantly different from null (0.17; 95% CI 0.09 to 0.26) as was that for model II (ERR at 100 mGy=0.16; 95% CI 0.07 to 0.26). Leave-one-out sensitivity analyses found one potential influential study (study no. 2). Excluding this study resulted in a modest increase (<25%) in the effect size for both models, resulting in ERR estimates of 0.21 (95% CI 0.11 to 0.33) and 0.21 (95% CI 0.09 to 0.35) for model Ib and model IIb, respectively. Subsequent removal of the next closest influential study (no. 1) resulted in ERR estimates of 0.25 (95% CI 0.08 to 0.46) and 0.34 (95% CI 0.04 to 0.72) for models Ic and IIc, respectively. Further excluding incidence studies resulted in ERR estimates of 0.25 (95% CI 0.07 to 0.46) and 0.35 (95% CI 0.02 to 0.79) for models Id and IId, respectively. Removing influential studies and restricting models to occupational studies provided similar results (model Ie: ERR at 100 mGy=0.24 (95% CI 0.06 to 0.44), model IIe: ERR at 100 mGy=0.30 (95% CI −0.01 to 0.70)). Removing influential studies and excluding log linear models resulted in ERR estimates of 0.24 (95% CI 0.06 to 0.45) and 0.34 (95% CI 0.01 to 0.77) for models If and IIf, respectively. There was little evidence of study heterogeneity as evidenced by the lack of between-study variance and Cochran's Q test probabilities near unity for all models (p value range: 0.73 for model Id to 0.98 for model IIb).
Meta-analysis results using random effects models
Results of planned sensitivity analyses
Publication bias
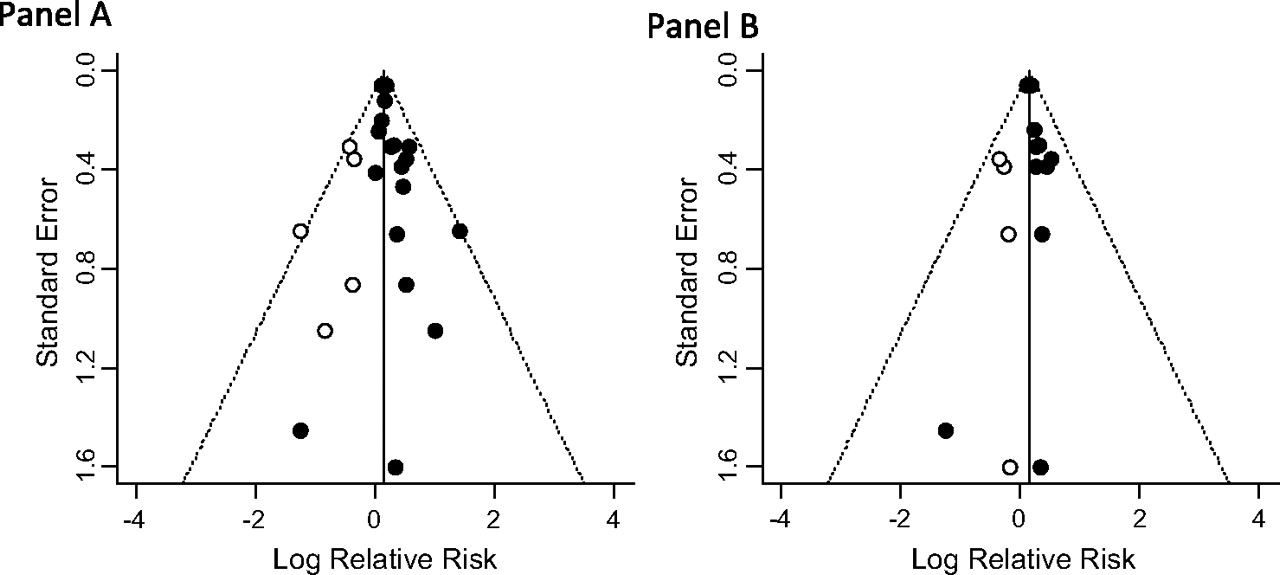
There was suggestion of publication bias in all models tested, as evidenced by consistent non-zero regression intercepts and fail-safe N values less than tolerance (table 2). Likewise, funnel plots indicated asymmetry among published studies (figure 2, filled circles). These plots also show the number and magnitude of missing studies that are necessary for symmetry. Trim and fill methods suggested that negative studies were missing from all variations of model I and models II and IIb (table 3). These methods suggested a slight adjustment in the opposite direction for model IId. Nevertheless, including missing studies in any model did not markedly affect estimates. Moreover, the fail-safe N was very large relative to the number of missing studies as well as the total number of studies in each modelling scenario. Therefore, there was little evidence of substantial publication bias.
{kind=link}
{kind=link}
Funnel plots for model I (panel A) and model II (panel B) showing the effect size versus standard error (log scale). Plot also shows the results' trim and fill analyses, that is, the actual studies (filled circles), the missing studies (open circles) and the 95% CI (dotted lines).
Discussion
Ionising radiation is a known and extensively studied human carcinogen. However, its effects at doses encountered in occupational and diagnostic medical settings remain a matter of much debate.43 44 In part, the disagreement stems from the difficulties in quantifying small risks using observational data. It is impractical in most settings to conduct a single epidemiological study that is sufficiently large to directly obtain precise estimates of risks at low doses.45 Furthermore, although the RR may be statistically significant, the absolute risk in the low-dose range is small and may be influenced by a host of external factors. Nevertheless, systematically combining the available information can reduce the effects of random error and provide a precise aggregate estimate.
We used a simple statistical approach to pool available information on the dose–response relationship between leukaemia and ionising radiation in a manner that is both quantitative and reproducible. Our estimates of the ERR at 100 mGy ranged from 0.15 (95% CI 0.07 to 0.23) for full model I adjusted for publication bias to 0.37 (95% CI 0.03 to 0.81) for model IId restricted to non-influential mortality studies also with bias adjustment. These estimates were in reasonable agreement with the leukaemia risk observed among males exposed as adults in the LSS cohort (ERR at 100 mGy=0.15; 95% CI −0.11 to 0.53) using the linear term in a linear-quadratic dose–response model.46 Unlike the LSS which reports risks from acute exposure to a wide range of doses, our models provided a precise and quantitative summary of the direct estimates of excess risk from studies of protracted occupational and environmental radiation exposures.
A possible explanation for the overall lack of between-study variance is that most studies were occupationally based and examined workers with similar jobs and eras of employment. Measurement data from personal dosimetry systems are often available for study participants from nuclear industries, leading to reduced uncertainties in exposures and avoidance of exposure misclassification that may bias results. Finally, leukaemia is an endpoint that has been shown to be relatively resistant to confounding or effect modification by exposures to other leukaemogens in epidemiological studies, as it has few known risk factors.23 42
Sensitivity analyses revealed that study no. 2 particularly influenced the aggregate estimate because of its small standard error compared to other studies in the analysis. Study no. 2 evaluated the leukaemia mortality risks associated with protracted exposures in Russian nuclear workers (n=21 557) employed at the Mayak complex between 1948 and 1972. The large study size and wide dose distribution increased the precision of risk estimates. The average cumulative external dose among the Mayak workers (810 mGy) was about 20-fold higher than most other studies under observation. Recent improvements in Mayak exposure estimates47 show a shift in the external dose distribution away from the higher exposures found in earlier studies,48 suggesting confirmation of exposure misclassification that would bias risk estimates toward the null. Other studies have made similar observations resulting in additional explanations for risk attenuation with moderate to high exposures: a healthy worker survivor effect, a depletion of the number of susceptible people in the population at high exposure levels, confounding by other risk factors that vary across levels of the main exposure, and saturation in the exposure–response relationship for biological processes involved in disease development.23 49–51 Regardless of the cause, risk attenuation at high doses may explain the reduction in the slope of the linear dose response observed in the Mayak cohort compared to cohorts with lower average cumulative exposures.
The next likely influential study was study no. 1. Hwang et al19 examined leukaemia incidence in a cohort of Taiwanese residents (n=6242) exposed between 1983 and 1992 from52 Co-contaminated reinforcing steel used to construct their dwellings.19 Only six incident leukaemias occurred in a cohort whose average excess cumulative exposure was less than 50 mGy (range: <1–2363). The precision of this study is remarkable given its size; studies of similar size and exposure characteristics were much less precise. This population-based study differs from most occupational studies in that the cohort is relatively young (mean age at first exposure was 16.9±16.5 years) and individual exposures were estimated without the availability of personal dosimetry measurements. However, these differences are unlikely to fully explain the observed disparity in study precision. The overall effect of choosing whether to exclude one or both outlying studies was small, suggesting that aggregate results are robust.
Limitations
Meta-analyses of cancer risk among low-dose radiation studies must consider sources and magnitude of bias within each contributing study. Each study possesses limitations in methods and available data that may contribute to bias. The major sources of bias for leukaemia risk in low-dose observational studies are (1) dose error and uncertainty and (2) exposure to other leukaemogens that is differentially distributed with respect to ionising radiation. With regard to the former, most studies of nuclear workers involve individual badge dosimetry, the magnitude of which has been quantified in recent studies.53 These errors have generally been found to be small ‘classical’ errors which would be more likely to cause bias toward the null.54 Environmental studies, by contrast, frequently involve exposures that are Berksonian in error and can have uncertain effects on risk estimates.54 Regarding the latter source, exposures to benzene, 1,3-butadiene, carbon tetrachloride, ethylene oxide, formaldehyde, and trichloroethylene are known (ie, benzene) or suspected to be linked to leukaemia.55 56 Of these chemicals, benzene is the only known leukaemogen likely to be associated with radiation exposures, and then only among worker-based studies. A previous pooled study found that inclusion of benzene slightly reduced radiation–leukaemia risk estimates.23 The risk estimate for this study (within this meta-analysis) is benzene-adjusted. Other worker-based studies, particularly those based on more recent employment, have found little evidence of potential benzene exposures, as this substance was never used or has been phased out of many workplaces.29 40 Unlike solid cancers, leukaemia is advantageous for meta-analysis because it is not strongly associated with lifestyle factors, although there is some evidence of a moderate association (RR=1.4–2.0) between smoking and some leukaemias.57–59 Given the small magnitude of the observed association, occupational radiation exposure and smoking would need to be highly correlated to account for even a modest effect on the dose–response trend for leukaemia.60 Nonetheless, the effects of smoking and concomitant leukaemogen exposures are largely unaccounted for in most studies, which is a limitation in our meta-analysis.52
Studies suitable for inclusion were limited to populations primarily exposed to low-LET radiations; however, concomitant exposures to neutrons and internally deposited alpha-emitters were likely in many situations. Some studies included high-LET exposures so that the effects due solely to low-LET exposures could not be examined.27 29 Thus, there is a potential for bias from limitations in adjusting for dose heterogeneity. However, recent studies of the relationship between low-LET irradiation and leukaemia have shown little effect from adjusting for plutonium exposures 20 23 and have also shown exposures to neutrons and alpha-emitting radionuclides are typically small relative to low-LET exposures.23 24 27 29 32–34 37 38 42 Therefore, a substantial bias from dose heterogeneity in selected studies is unlikely.
Three primary studies (13%) reported results from log-linear dose–response modelling.19 24 38 We assumed that risk estimates from log-linear and linear models using these data would be similar at low doses (ie, <100 mGy) because dose ranges did not appear great. However, the uncertainty between these models may substantially differ. Our sensitivity analyses revealed little evidence that the log-linear model results had a strong effect on the aggregate estimates as shown by models If and IIf. Thus, our estimates of ERR at 100 mGy as a risk per 100 mGy may be reasonable at exposures below this level, but caution should be used when extrapolating above this level.
Obtaining sufficient information to estimate study precision was problematic. It was common for studies to report uncertainty using confidence intervals calculated from profile likelihood methods, and the distribution of the likelihood function was unknown. Reported confidence intervals were often asymmetric and were sometimes reported as inestimable due to parameter space constraints of the model. We were able to obtain the original estimates of standard errors for seven studies. Comparing our estimates to reported standard errors suggested that our methods slightly overestimated standard errors. Replacing our estimates with reported values or adjusting to account for an observed bias did not noticeably change the aggregate estimate (data not shown). Thus, there is little evidence of a significant bias due to inadequate estimation of the standard errors. However, more work is needed to examine the coverage of confidence intervals for the aggregate estimates.
Although we observed little change in estimates following adjustment, there was evidence of publication bias away from the null. It is likely that smaller and earlier studies lacked the statistical power needed to perform informative dose–response analyses. Of 15 studies that were superseded by studies with improved follow-up, seven (47%) reported negative ERR values. Moreover, some larger studies included dose–response modelling only if an elevation was observed in other comparisons (eg, standardised mortality ratio (SMR), standardised rate ratio (SRR)).61 Our analysis suggests that model II results were the least affected by publication bias. We propose this bias was minimised because the large pooled studies used in model II included many small cohorts that likely had null or negative values, which may not have been published individually with dose–response estimates. We reported results following an adjustment for publication bias in some models, although publication bias cannot be confirmed without uncovering the actual ‘negative’ unpublished studies. We advise cautious interpretation of tests of heterogeneity and bias in our meta-analysis as there is no statistical test that can confirm or exclude bias with certainty.
We excluded CLL from our analysis because information on CLL risks was sparse among the studies examined. However, we note that CLL radiogenicity is the subject of recent enquiry.62–66 The majority of information obtained for our analysis resulted from mortality studies that may underestimate risks due to improved survival in leukaemia patients. Furthermore, several studies acknowledged difficulty in case ascertainment, most notably among incident and environmental studies. Thus, a potential bias may exist from underascertainment of incidence cases.
Conclusion
Occupational and environmental epidemiological studies are, in principle, preferred over studies of high-dose exposures for estimating the effects of low-dose protracted ionising radiation exposures. Unfortunately, these studies have individually lacked the precision necessary for the projection of population-based risks. Using a simple meta-analytical approach to synthesise the available information, we found that leukaemia (excluding CLL) is significantly associated with exposure to protracted, low-level ionising radiation. Our preferred estimate of leukaemia risk at 100 mGy is 0.19 (95% CI 0.07 to 0.32), achieved by combining information from existing pooled analyses and non-overlapping studies, excluding one influential study, and adjusting for publication bias.
We found between-study effects to be minimal, which suggests that differences in study populations and epidemiological methods were essentially unimportant. Although publication bias was indicated, subsequent adjustment did not markedly change aggregate estimates. Likewise, excluding influential studies resulted in only moderate effects on risk estimates. In fact, all model results were in reasonable agreement with the leukaemia risk observed in atomic bomb survivors, which is regarded by most as the gold standard. Thus, our results appear robust and strengthen our confidence in the current understanding of leukaemia risk among populations exposed to ionising radiation.
References
Footnotes
See Editorial, p 387
Disclaimer The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the National Institute for Occupational Safety and Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.